HCG / Human Chorionic Gonadotropin for Male Infertility

Introduction to HCG / Human Chorionic Gonadotropin for Male Infertility
Luteinizing hormone (LH) is the hormone from the pituitary gland which tells the Leydig cells in the testicles to make testosterone. Human chorionic gonadotropin (HCG) is a medication which has a similar structure and essentially the same hormonal action as LH. However, HCG has a much longer half-life (30 hours) than LH (30 minutes), with a peak onset of increased testosterone of about 72-96 hours after administration. [Madhusoodanan V. IBJU 2019] Since HCG works by increasing LH activity, if the LH is already elevated (over 20 IU/L) then HCG will likely not be effective at increasing testosterone levels.
Like SERMs and anastrazole, HCG works to increase endogenous production of testosterone. It is considerably more expensive than the two oral medications and must be given by injection (typically 3 times per week subcutaneously). The primary potential advantage of HCG over SERMs is that it does not require a functioning pituitary gland to work effectively. Therefore in men who have a non or poorly functioning pituitary along with low testosterone levels may benefit from the use of HCG. Permanent pituitary dysfunction can be congenital (e.g. Kallmans Syndrome) or result from local tissue destruction from a pituitary tumor or prior surgery/radiation to the area. Temporary decreases in pituitary function commonly occurs with the use of exogenous androgens which suppress pituitary release of FSH and LH. Even after stopping the androgens it can take some time before the pituitary will respond adequately to SERMs in terms of increasing LH (and therefore testosterone) levels.
However, it can sometimes be more effective when the pituitary gland is not responding to clomiphene, and is generally able to raise testosterone levels higher than can anastrazole (as long as baseline LH levels are not elevated above 20 IU/L). Like clomiphene, HCG can increase estradiol to abnormally high levels in some men through the conversion of testosterone to estradiol by the aromatase enzyme.
A common question is whether HCG is more effective than SERMs or anastrazole in treating male infertility. Remember that these medications do not directly improve sperm quality, but rather exert their effect by increasing testosterone production (and, in the case of SERMs and anastrazole, possibly FSH levels if these are low). Therefore, a man whose testosterone is pushed back up into the normal range by either SERMs, anastrazole, or HCG should have the same potential clinical benefit to sperm quality. HCG may be more effective in men who still have low testosterone levels on SERMs but whose LH is still not significantly increased (indicating an inadequate response by the pituitary gland to the SERM). Another difference is that, unlike clomiphene and anastrazole, HCG does not increase FSH production, although this should not matter clinically in men whose FSH is already elevated.
COMMERCIAL AVAILABILITY OF HCG
Commercially, HCG comes in several different formulations. In men Pregnyl, and Novarel are most commonly used, but generic HCG is also made by compounding pharmacies. The three are essentially equivalent in terms of dosing and potency. All three of these medications use HCG extracted from the urine of pregnant women. Other forms of HCG that are less commonly used in men include Ovidrel, Follutein, Profasi, Choragon, and Choropex. Note that blood LH levels often do not increase in men taking HCG, as the exogenous hormone does not display much cross-reactivity with most commercial laboratory assays.
HCG is not available at most local pharmacies due to a nationwide shortage, and typically needs to be ordered through specialty pharmacies. The shortage is attributed to the popularity of HCG as a weight-loss supplement, despite controlled studies failing to show any evidence that HCG use actually enhances weight loss. Currently, the FDA deems as fraudulent the marketing of HCG as a weight loss enhancement. The popularity of HCG has also risen through its use by “rejuvenation” clinics for men seeking an improved quality of life and/or sexual function, as well as body builders, who often use HCG between cycles of anabolic steroid use to maintain testicular function. A 2019 FDA ruling has also made HCG unavailable by most compounding pharmacies, which has served to further worsen the shortage of HCG in the United States.
HCG may be covered by your insurance company, but if you do not have insurance coverage for your medications, the pricing of HCG from some regional and fertility-specific pharmacies is reviewed in the "Fertility Medications Cost" section of this website.
HOW HCG IS USED
HCG must be given by injection, either intramuscular (IM) or subcutaneous (SQ). Protocols for injection schedules differ, but most experts recommend three times per week.
HCG can be given in 2 ways: high dose or low dose:
Low Dose HCG
Studies have shown that low dose HCG (500 IU SQ 3 times per week) was adequate to maintain normal intratesticular levels of testosterone. [Coviello AD. JClEndoMet 2005]. By itself, this low dose HCG is not enough to keep good circulating blood levels of testosterone and also does not address adequate FSH stimulation of the spermatogenic cells for good sperm production. However, a combination of testosterone replacement therapy (exogenous androgens) combined with low dose HCG and injectable FSH is adequate in maintaining good sperm production in most men. Of note, injectable FSH is necessary in this situation as SERMs/anastrazole will not stimulate FSH production from the pituitary in the face of TRT.
High Dose HCG
The goal of high dose HCG is to maintain good blood levels of testosterone while also maintaining adequate intratesticular T levels as well. Dosages can range from 1000 IU to 4000 IU three times per week. For men who are just stopping the use of high dose exogenous androgens, I generally start at a dosage of 3000 IU SQ 3 times per week (with the addition of a SERM to try and speed up recovery of FSH production).
After starting high dose HCG it is always important to check repeat hormone testing 2-4 later. Labs to always check include total testosterone (goal 500-1000 ng/dL), estradiol (goal <60 pg/mL and T/E ratio ³ 10:1) and hematocrit (goal <54%). Possible additional labs include a prolactin (if baseline testosterone was <300 ng/dL) and FSH if low at baseline and you are trying to stimulate production with a SERM as well. Once hormonal levels are normal, I typically repeat labs (testosterone, estradiol, hematocrit) 6 months later, and then every 12 months while the man is taking the medications. Any change in hormone medication or dosage should generally have repeat labs 2-4 weeks later to make sure that there was the appropriate change in the corresponding hormones.
SIDE EFFECTS of HCG
Most men taking HCG do not have any adverse side effects and multiple studies have concluded that it is a safe and effective treatment for hypogonadism. [Lee JA. TranslatAndrolUrol 2018]. A study of 175 men taking HCG injections found that none of them had any significant adverse side effects. [Tsujimura A. TheAgingMale 2005]. No side effects or complications were also seen in a study of 20 men taking HCG for hypogonadism. [Madhusoodanan V. IBJU 2019]
Rare potential side effects include headaches, weight gain, hypertension, cataracts, acne, dizziness, restlessness, insomnia, mood changes (depression, irritability) and pain at the injection site.
Breast tenderness and/or enlargement (gynecomastia) can occur but should be rare if estradiol levels are monitored and kept within the normal range.
Hematocrit Levels
Increases in hematocrit have been noted in men taking HCG injections, though rates of polycythemia are low. [Tsujimura A. TheAgingMale 2005]. I recommend monitoring hematocrit levels with a goal to keep the hematocrit at 54% or less. For more information see the website section “Erythrocytosis/Polycythemia”
Use With Other Hormonal Medications
HCG is commonly used with anastrazole in the treatment of hypogonadism, since they work on increasing testosterone levels by different mechanisms. Men with elevations in their estradiol levels while taking HCG may also benefit from the aromatase-inhibiting activity of anastrazole as well. SERMs and HCG both work by increasing LH-effect, so these medications are not commonly used together (unless the SERM is being utilized to increase an inappropriately low FSH level, such as men just coming off TRT). Low-dose HCG can also be used by men on exogenous androgens to maintain some basal testicular function. For more information on this, see the “Exogenous Androgens/Anabolic Steroids” section of this website.
HCG Injection Instructions
HCG can be given either subcutaneously (SQ) or intramuscularly (IM). Both of these are felt to be equally effective, but the SQ approach uses a smaller needle size and is felt to be more comfortable. On rare occasions, a patient who is not responding as expected to SQ HCG injections may have a better effect with trying IM injections of HCG.
Basic injection teaching videos can be found at: www.villagefertilitypharmacy.com
Go to “Medication Injection Lessons” in right upper corner
Scroll down and click on “HCG”, “Novarel”, or “Pregnyl” (whichever you have been prescribed)
Most commercial formulations of HCG (e.g. Pregny and Novarel) come in 10,000 unit vials that need to be mixed by the patient prior to use. Some compounding pharmacies send HCG in different size vials (up to 50,000 IU). These pharmacies will need to provide you with individualized instruction on how much HCG to inject depending on your prescribed dosage.
The following are some basic instructions for men taking HCG using a standard 10,000 IU vial.
The HCG will come as a powder inside a sealed bottle. This powder is mixed with a sterile fluid called ‘diluent’, into which the HCG powder dissolves. The appropriate amount of fluid is then taken into a syringe and is injected subcutaneously into the upper outer thigh, lower abdomen, or upper outer arm region (as shown in the “Subcutaneous Injection Lessons” video on above listed website). The dosing instructions for the video directions are designed for women who typically use the entire vial (10,000 IU) in one injection to trigger ovulation. So, although the injection techniques are the same, slight modifications need to be made for males who typically use the HCG three times a week for prolonged periods of time.
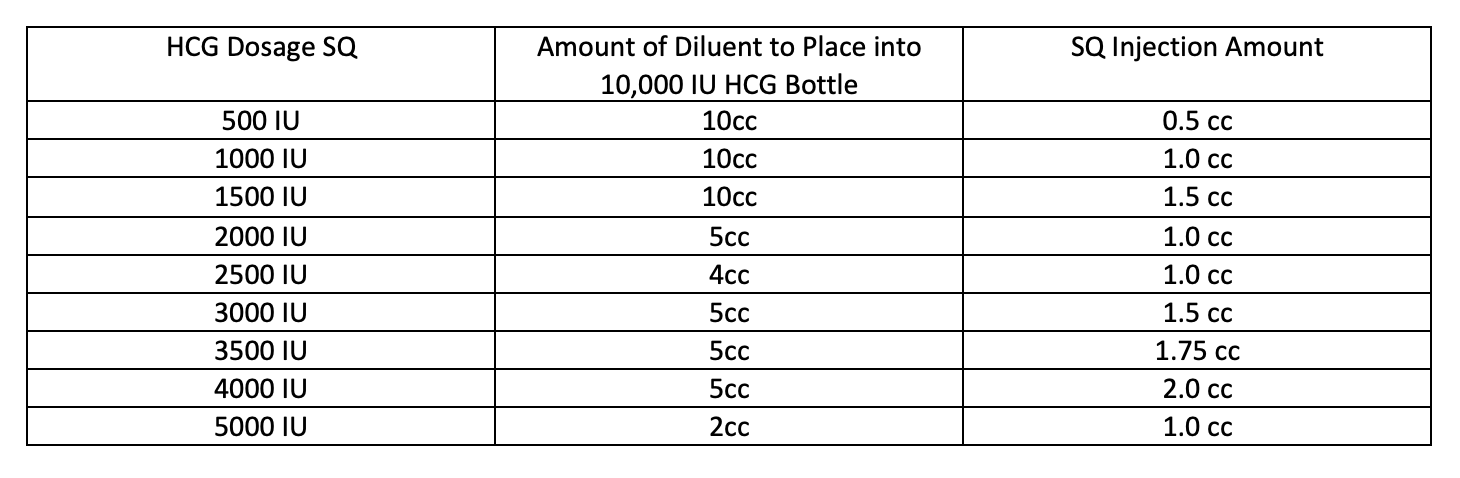
In general, 1cc to 2cc are generally used for SQ injections (more than this can cause an uncomfortable raised area at the injection site). Each vial of powder contains 10,000 IU of HCG. The amount of fluid that needs to be injected depends on the amount of diluent used to dissolve the powder. The amount of diluent used can be modified according to the dose of HCG being used. The following chart gives the recommended diluent and injection amounts for each dosage.